As clinicians, we often hear the acronym
LGBTQIA+ in reference to those with a variety of gender identities and sexual orientations. But are you aware of what those letters stand for? The abbreviation refers to various gender identities and sexual orientations including Lesbian, Gay, Bisexual, Transgender, Queer/Questioning, Intersex, and Ally. The ‘+’ in the acronym can include various other identities including pansexual, demigirl, demiboy, gender non-binary, gender non-conforming, gender fluid, asexual, and aromantic. As this is a growing field, new identities and terms are emerging, and it becomes essential for clinicians and medical professionals to educate ourselves in order best help our clients and families.
What is sexual orientation? It is an individual’s preference of sexual partners. Is sexual orientation just sexual attraction? Research shows that sexual orientation is not only sexual attraction, but also sexual identification and sexual behavior. All three components generally align well and are significantly correlated. However, one’s identity and behavior can vary for a variety of reasons including political, religious, opportunities, culture, and parental/societal expectations.
Ultimately, what determines your sexual orientation? Is it determined in the mother’s uterus and is biological? Do we have a ‘gay gene’? Or could it be a change in the brain?
IN THE MOTHER'S UTERUS
Research suggests that a person’s sexual orientation is determined biologically when a child is in their mother’s uterus. Varying amounts of sex hormones at varying times in prenatal (pre-birth) development influences a person’s gender and sexual orientation.
Human sexual hormones include testosterone, estrogen, progesterone and other related hormones. In research completed on animals, it was identified that biological sex, i.e., being male and female is influenced by changes in prenatal testosterone. This was found through animal studies that have shown that by injecting sex hormones, such as testosterone at various stages of development, there are changes to specific parts of the brains and bodies of these animals. These changes depended not only on the amount of testosterone injected but also on the timing of the injections.
Since sexual orientation is a gendered trait, meaning that sexual orientation is a part of gender, current research on the development of sexual orientation is primarily focused on prenatal sex hormones. Based on animal studies, it is likely that the critical period for sex hormones in humans is pre-birth. Prenatal sex hormones are found to influence gender and gendered traits, so it is safe to assume it also influences sexual orientation.
While such studies have been conducted in animals, it is unethical to inject sex hormones into human fetuses in the uterus. So how do we know that sex hormones influence gender and sexual orientation in humans? Researchers study conditions that mimic the studies in conducted in rats. One such condition, called Congenital Adrenal Hyperplasia (CAH) which is a disorder that causes the adrenal gland to secrete excess testosterone during prenatal development in pregnant women. Children of these women with CAH are significantly more likely to be homosexual compared to the children of women without this condition.
Since sexual orientation is one aspect of gender, it can be assumed that human sexual orientation is also influenced by changes in testosterone and other sex hormones during prenatal stages of development.
According to a presentation by C&A’s Doctoral Intern Sushmitha Mohan, “same-sex attraction is a part of a package of gender a-typical traits.” She emphasized that sexual orientation is an aspect of gender that emerges from prenatal sexual differentiation in the brain, which is influenced by their genes, sex hormones and brain systems,” said Mohan. This implies that sexual orientation is a biological trait that is determined when the fetus is developing in the mother’s uterus.
Mohan also presented that there were structural and functional differences in brains and bodies of gay and straight people, which may also be influenced by the prenatal levels of sex hormones. According to research, some characteristics of the bodies and minds of gay men are shifted in a straight female direction compared with straight men, and some characteristics of the bodies and minds of lesbians and bisexual women are shifted in a straight male direction compared with straight women. These shifts are identified in specific traits and do not indicate gender reversals. It’s important to also keep in mind that these shifts occur in only a few gendered traits (e.g., the lengths of fingers), and do not influence all gendered traits.
DIFFERENCES IN THE BRAIN AND BODY
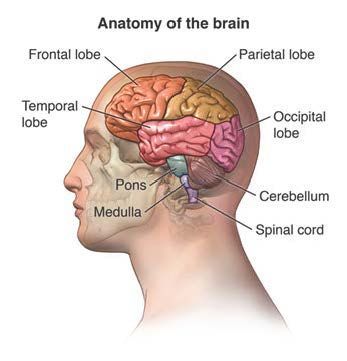
The human brain is essentially gendered, meaning that male brains are typically different than female brains in various ways. However, studies show that the brains of gay men and women are more similar to the brains of the opposite gender in a few specific ways. Some of these changes are in parts such as the hypothalamus and anterior commissure.
In humans, the hypothalamus is approximately the size of a pea. The hypothalamus is a gland in your brain that controls the hormone system. It releases hormones to another part of the brain called the pituitary gland, which sends hormones out to your different organs. The anterior commissure is a bundle of nerves connecting the two temporal lobes.
Studies that examined the differences between gay and straight men and women found that the brains of gay men were similar to straight women in some ways, and the brains of gay women were more similar to that of straight men in some ways. For example, the anterior commissure, which is typically larger in women than men, was found to be larger in gay men than straight men. In a different study, the corpus collosum was found to be significantly larger in gay men than straight men, which is more typical of female brains. Similarly, parts of the hypothalamus (a cell cluster called INAH3) was found to be gender shifted for gay men. Other gender shifted brain differences include the sizes of hemispheres of the brain, and differences in lateralization.
Some studies have also identified finger length ratios, known as the 2D:4D ratios, to be different between gay people and straight people. This ratio is the length of the index finger divided by the length of the ring finger. Straight males typically have a lower 2D:4D ratio and straight females have a higher 2D:4D ratio. Several studies have found that lesbians have lower ratios (more male liken ratios) and that gay men have higher ratios (more female like ratios).

DOES BEING GAY RUN IN FAMILIES?
The short answer is Yes! Gay men and women are more likely to have gay siblings than straight men and women. Typically, about seven to 16% of the same sex siblings of gay people are found to be gay.
There are a few reasons for family clustering, including genetics. Studies show increased rates of homosexuality or bisexuality among non-sibling relatives of gay or bisexual people, and increased rates in same-sex siblings vs. opposite sex siblings. In twin studies, there is a 50% concordance rate in identical twins and 30% concordance rate of homosexuality in non-identical twins. Research also suggests that it is the maternal inheritance of genes that predispose males to same-sex attraction. In addition, it is identified that it one gene in chromosome-8 could influence homosexuality in men.
Another interesting study showed that gay men, on average, have more brothers than straight men. However, the influence of older brothers is not a direct one but hypothesized to be mediated by their mother (her immune system). This theory proposed that mother’s immunization against male-specific antigens changes during each pregnancy, which could affect changes in sex hormones in pregnancy, and thus sexual orientation.
DO GAY PARENTS RAISE GAY CHILDREN?
It should be noted that the vast majority of gay people have straight parents. Studies show that children raised by gay parents do not differ from average in any single developmental/cognitive characteristic when compared to children raised by heterosexual parents.
If your child is struggling with self-identification or orientation, please call C&A at 330.433.6075. One of our caring clinical staff members will provide help for families.
C&A Doctoral Intern Sushmitha Mohan presented the information for this blog post at an agency training on Feb. 18. Mohan’s doctoral internship with C&A will end on June 30, 2022.
RECENT POSTS