The holiday season just ended with fewer social gatherings and parties and increased isolation due to the COVID-19 pandemic may lead some people to seek comfort in having an adult beverage. But if you are pregnant or perhaps are not even aware you are pregnant, one glass of wine today, could lead to a whole host of problems later.
Fetal Alcohol Spectrum Disorders (FASD) is the result of a pregnant woman having one or more drinks during pregnancy. Child and Adolescent Behavioral Health's FASD Clinic Supervisor Dr. Marysa Williams wrote, “No amount of alcohol has been proven safe at any time during pregnancy. You should not drink alcohol if you are pregnant, trying to get pregnant or think you may be pregnant. There’s really no safe time to drink alcohol during pregnancy. Alcohol can cause problems for your baby. Many women are not even aware they are pregnant in the first six weeks.”
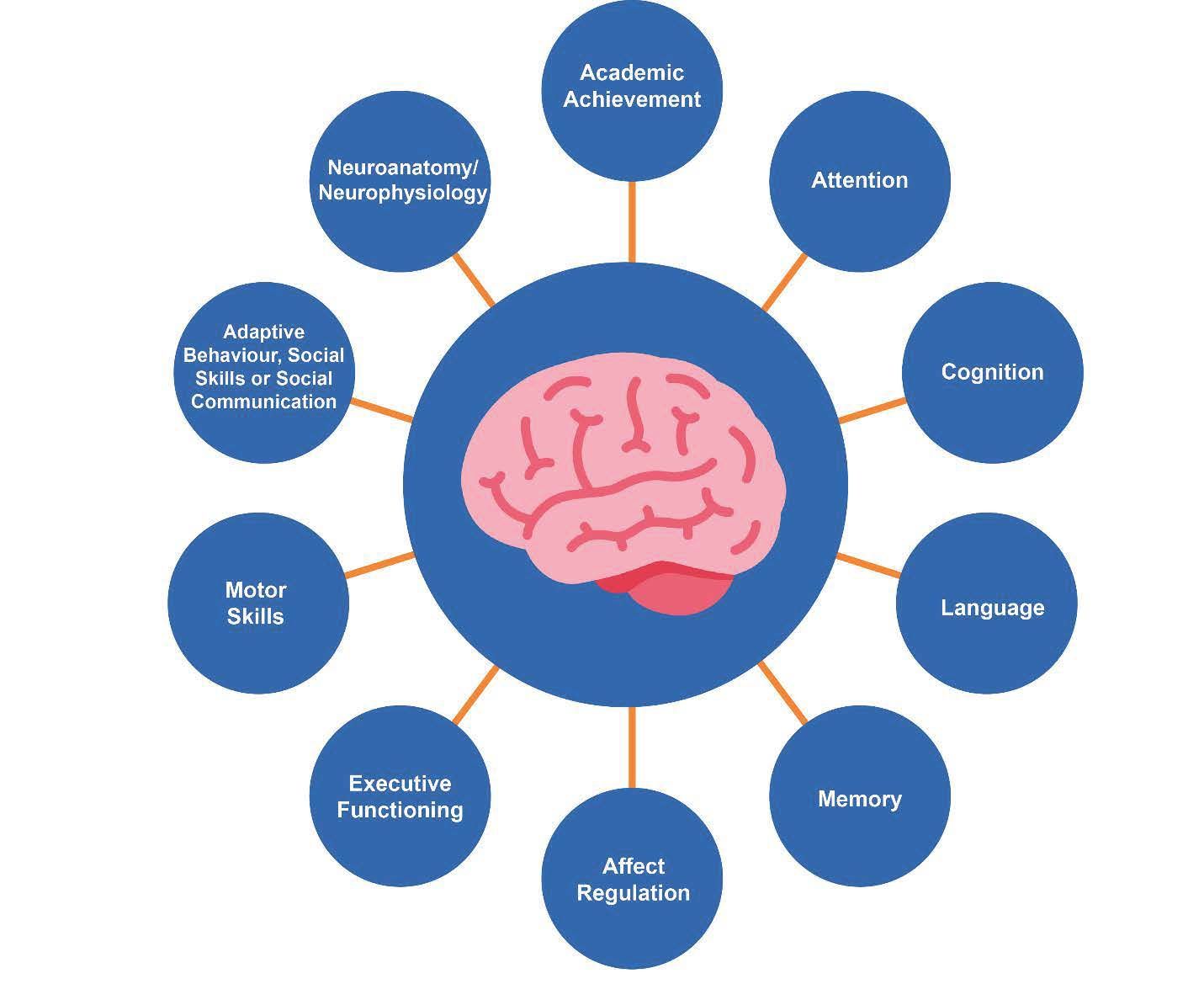
Of course, alcohol is not the only substance that can cause an issue for women during pregnancy. Any substance consumed during pregnancy plays a role in a child’s development. “Studies show that using drugs – legal or illegal – during pregnancy has a direct and potentially negative impact on the baby,” wrote Dr. Williams. “However, the only known cause of Fetal Alcohol Spectrum Disorders (FASD) is prenatal alcohol exposure. Alcohol is a teratogen that crosses the placenta and can damage the central nervous system (including the brain) and other organs of the developing baby. Other substances when taken during pregnancy increases the chances of birth defects, premature babies, low birth weight and miscarriage.”
WHAT ARE THE SIGNS OF FASD?
Prenatal alcohol exposure can cause a number of birth defects, including microcephaly, a condition in which the baby’s head and brain are significantly smaller than expected, abnormal facial development in the lip, mid-face, eyes and structural brain defects.
A child with FASD may have:
- Low body weight
- Poor coordination
- Hyperactive behavior
- Difficulty with attention
- Poor memory
- Difficulty in school (especially math)
- Learning disabilities
- Speech and language delays
- Intellectual disability or low IQ
- Poor reasoning and judgement skills
- Sleep and sucking problems as a baby
- Vision or hearing problems
- Problems with heart, kidneys or bones
- Shorter-than-average-height
- Small head size
Abnormal facial features, such as a smooth ridge between the nose and upper lip (this ridge is called the philtrum)
HOW IS CHILD DIAGNOSED WITH FASD?
Child and Adolescent Behavioral Health is one of the three FASD clinics in the state of Ohio and the only clinic in Northeastern Ohio. The other two clinics are located in Toledo and Cincinnati.
C&A’s Belden Office facilitates the FASD Clinic. Dr. Williams explained how a child is diagnosed with FASD at C&A, “FASD is diagnosed by a team of interdisciplinary professionals, gathering information and assessments in four specific areas: growth, facial features, brain function and structure, and prenatal alcohol history.”
If a child is diagnosed with FASD, they may be classified under one of the four umbrella terms.
- FAS (Fetal Alcohol Syndrome)- People with FAS have the most severe central nervous system (CNS) dysfunction, the presence of the classic characteristic facial features, significant growth deficiency and confirmed severe prenatal alcohol exposure.
- PFAS (Partial Fetal Alcohol Syndrome)- The term “Partial FAS” is used when a person’s characteristic features are very close to the classic features of FAS and the alcohol history strongly suggests that alcohol exposure during pregnancy was at high level and likely to have played a role in person’s difficulties.
- ARND (Alcohol Related Neurobehavioral Disorder)- This is the most common diagnosis on the spectrum. People with ARND have some but not all of the characteristic growth deficiency, characteristic facial features, and CNS damage/ dysfunction, but a number of other factors could be contributing to the present issues. Present issues may be genetic background, other potential exposures or problems during gestation, and various experiences since birth.
- ARBD (Alcohol Related Birth Defects)- This is the least common diagnosis on the spectrum. These individuals have the growth deficiency and/or facial characteristics that to some extent are compatible to FAS, but do not have clear evidence of cognitive or behavioral problems that strongly suggest CNS damage/ dysfunction.
If a child falls under one of the umbrella terms, is there a treatment for each one? Dr. Williams said, “FASD conditions are life-long. There is no cure for FASD, but research shows that early intervention treatment services can improve a child’s development. There are many types of treatment options, including medication to help with some symptoms, behavior and education therapy, parent training and other alternative approaches. No one treatment is right for every child. Each child with FASDs have unique strengths and challenges, but they all share the same basic needs and desires we all do: to be cared about, to be heard and understood, to make a difference, and to contribute to their families and communities. Helping a person to live successfully with FASD means recognizing strengths and focusing on ability over disability. Good treatment plans will include close monitoring/supervision, follow-ups, flexibility/changes as needed along the way, and needing to frequently repeat and rehearse skills.”
As previously mentioned, FASD may affect a child’s performance in school. Some common challenges for educators who teach students with FASD include hyperactivity, impulsivity, attention and memory deficits, difficulties with completing tasks, disruptive behaviors, difficulties with social skills, and the need for constant supervision and close monitoring.
Successful strategies for educating children with FASD include using concrete, hands-on learning methods, establishing structured routines, keeping instructions short and simple, providing consistent and specific directions, frequently repeating instructions and rehearsing tasks, and providing constant supervision.
Once strategies and coping skills are mastered, the next step is helping a person to live successfully with FASD. As mentioned previously, this means recognizing strengths and abilities of the person, rather than overly focusing on deficits and challenges. The focus should be on competencies, relationship mutuality and working with, rather than talking at the teen/ young adult. We all require help from others in varying degrees and most of us live interdependently in our communities. The focus for individuals with FASD should be on interdependence to support success.
PERCENTAGES OF CHILDREN AFFECTED FASD?
Each year, there is an estimated 40,000 babies born that are affected by FAS (Fetal Alcohol Syndrome) or FASD, with damage ranging from major to subtle.
One in 100 babies have FASD, nearly the same as autism. FASD is more prevalent than Down Syndrome, Cerebral Palsy, SIDS, Cystic Fibrosis and Spina Bifida combined. Alcohol use during pregnancy is the leading preventable cause of birth defects, developmental disabilities and learning disabilities.
If you live in Stark County, there are available resources. Those resources are Stark County Fetal Alcohol Spectrum Disorders Committee, Stark County Board of Developmental Disabilities and this website –
https://www.nofas.org.
HOW DOES A PARENT GET AN APPOINTMENT FOR THE CLINIC?
The waiting period before a first appointment is offered is variable, especially as the clinic only serves one client per month. Additionally, it is important to note that prior to becoming eligible for a first appointment, families must complete all necessary paperwork and obtain all necessary previous treatment records. Currently, we have several clients interested in services, but have not completed all necessary paperwork, and thus there may be immediate openings.
If you are interested in the assessment services provided by the FASD clinic, please talk to your provider at C&A about making a referral. If you are a new client, and do not have a C&A provider, please contact Meredith Skotschir, R.N., B.C., at 330-433-6075 ext. 227.
Psychology Doctoral Internship Program Manager Dr. Marysa Williams does testing and evaluation for the FASD Clinic, which is funded by the United Way. Dr. Williams is a licensed psychologist and one of C&A’s expert clinicians with over 4 years of experience. For more information about any of C&A’s services, call 330-433-6075.
RECENT POSTS